
Your kidneys have stopped working. Now you face a choice that will define your daily routine for years to come: hemodialysis or peritoneal dialysis. It’s not just a medical decision; it’s a lifestyle overhaul. One option requires visiting a clinic three times a week for hours at a time. The other turns your home into a treatment center with daily tasks. Both save lives by filtering waste from your blood when your kidneys can’t. But they do it in completely different ways.
If you’re reading this, you or someone you love is likely navigating End-Stage Renal Disease (ESRD). The anxiety is real. You want the best survival odds, but you also want to keep some semblance of normal life. This guide breaks down the hard facts about these two therapies so you can talk to your nephrologist with confidence.
How Each Therapy Actually Works
To choose between them, you first need to understand the mechanics. They both achieve the same goal-cleaning your blood-but the machinery involved is vastly different.
Hemodialysis uses an artificial kidney machine to filter blood outside the body. A machine pumps your blood through a filter called a dialyzer. Waste and extra fluid leave your blood and enter a cleaning solution called dialysate. Your clean blood then returns to your body. This happens via a vascular access point, usually an arteriovenous (AV) fistula created in your arm. The process is intense and fast, typically running at flow rates of 300-500 mL/min.
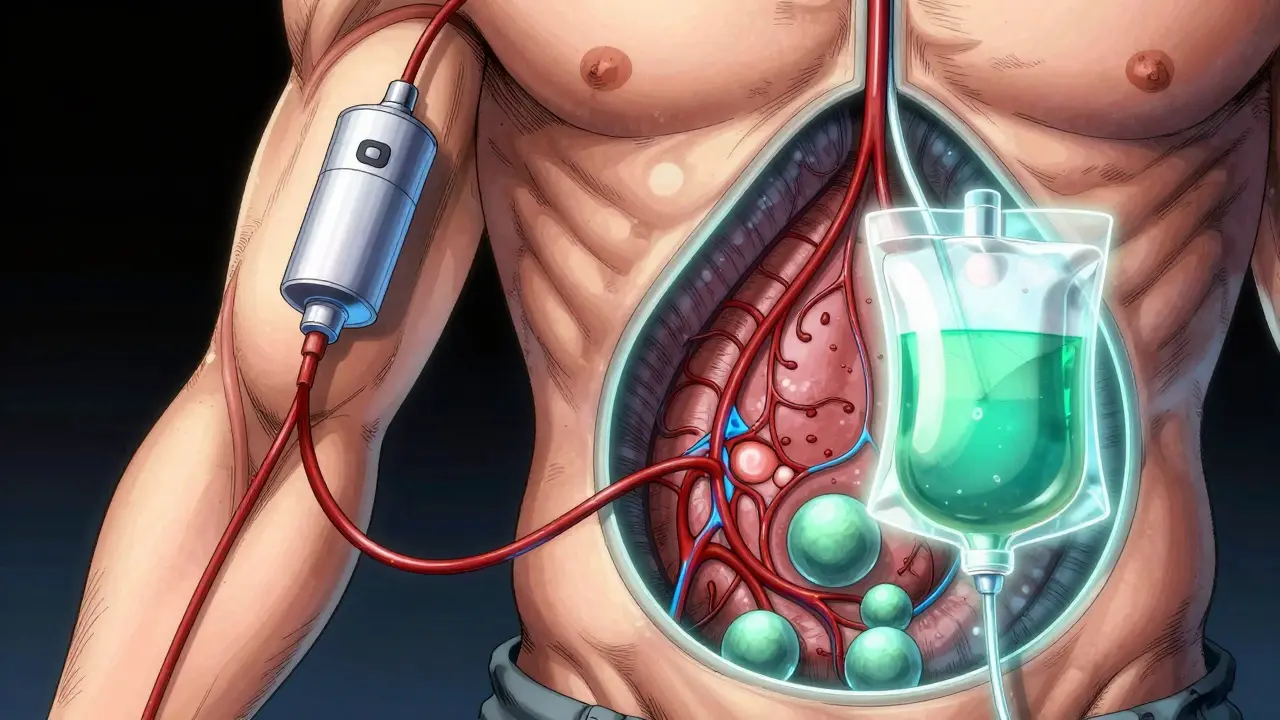
In contrast, Peritoneal Dialysis uses the lining of your abdomen as a natural filter. A soft tube called a Tenckhoff catheter is surgically placed in your belly. You fill your abdominal cavity with dialysate fluid. Your peritoneum acts as a semipermeable membrane, pulling waste and fluid from your blood vessels into the bag. After several hours, you drain the used fluid out and replace it with fresh fluid. No machines pump your blood directly. It’s continuous and gentle.
| Feature | Hemodialysis (HD) | Peritoneal Dialysis (PD) |
|---|---|---|
| Filter Mechanism | External machine (dialyzer) | Internal membrane (peritoneum) |
| Access Site | Arm (AV Fistula/Graft) | Abdomen (Catheter) |
| Frequency | 3 times per week | Every day (7 days a week) |
| Duration | 3-5 hours per session | Continuous or overnight cycles |
| Location | Clinic or Home | Home only |
The Daily Reality: Time and Flexibility
This is where most people make their choice. Let’s talk about your Tuesday morning.
With in-center hemodialysis, your Tuesday starts with a drive to the clinic. You sit in a chair for four hours while nurses monitor you. You can read, sleep, or watch TV, but you are tethered to the machine. When you leave, many patients report feeling "wiped out" for hours due to rapid fluid shifts. According to patient discussions on forums like Reddit, nearly 83% of HD users describe this post-treatment fatigue. You get weekends off, but your weekdays are rigidly structured around the clinic schedule.
With peritoneal dialysis, there is no clinic visit. You perform exchanges at home. If you choose Continuous Ambulatory Peritoneal Dialysis (CAPD), you do manual exchanges three to five times a day, taking about 30 minutes each. If you use an Automated Peritoneal Dialysis (APD) cycler, you hook up to a machine before bed, and it does the work while you sleep. You wake up free. The trade-off? There are no days off. Dialysis happens every single day, including holidays. You must always have dialysate bags nearby.
Who wins on flexibility? It depends on what you value. Do you prefer big blocks of free time on weekends (HD)? Or do you prefer small, manageable tasks spread throughout the day without leaving home (PD)? For travelers, PD can be easier if you plan ahead, as you can carry supplies. HD requires finding a partner clinic in every city you visit, which can be a logistical nightmare.
Health Outcomes: Blood Pressure and Survival
You might wonder if one method keeps you alive longer. The short answer is: neither has a consistent survival advantage in the general population. However, they affect your body differently.
A 2023 study published in the National Center for Biotechnology Information (PMC10626077) compared clinical outcomes directly. It found that PD patients had significantly better control over blood pressure and lower levels of parathyroid hormone compared to HD patients. Why? Because PD removes fluid slowly and continuously. HD pulls fluid out quickly, which can cause sudden drops in blood pressure and stress on the heart. This makes PD superior for hemodynamic stability.
PD also tends to preserve residual kidney function longer. Keeping even a little bit of your own kidney activity helps balance electrolytes and reduces dietary restrictions. HD, being more aggressive, can sometimes accelerate the loss of any remaining function.
However, HD is faster at clearing toxins in a single session. If you have acute kidney injury or severe fluid overload that needs immediate correction, HD is often the safer initial choice. For long-term chronic management, especially if you have heart issues, PD’s gentler approach may reduce cardiovascular strain.
Risks and Complications: What Could Go Wrong?
No therapy is risk-free. Understanding the specific dangers helps you prepare.
- Peritonitis: This is the biggest fear for PD patients. It’s an infection of the abdominal lining caused by bacteria entering during exchanges. Strict sterile technique is non-negotiable. Infection rates range from 0.3 to 0.7 episodes per patient-year. If you catch it early with antibiotics, it’s treatable. If ignored, it can damage your ability to do PD forever.
- Vascular Access Issues: HD relies on your AV fistula staying open. Clots, stenosis (narrowing), or infections at the needle site are common. You may need minor surgeries to keep the access working. Central venous catheters (used if a fistula isn’t possible) carry higher risks of bloodstream infections.
- Hernias: PD increases pressure in the abdomen, which can lead to hernias, especially if you lift heavy objects. About 10-20% of PD patients develop a hernia over time.
- Hypotension: Low blood pressure during HD sessions is common because fluid is removed too fast. This causes cramping, nausea, and dizziness.
If you have poor manual dexterity (like severe arthritis) or vision problems, PD’s requirement for precise connection of tubes might be challenging. Conversely, if you have extensive abdominal scarring from previous surgeries or morbid obesity (BMI >35), PD may not be suitable because the fluid won’t distribute evenly.
Cost and Insurance Coverage
In the United States, Medicare covers both therapies fully under Part B. However, the out-of-pocket costs differ.
PD is generally more cost-effective for healthcare systems. You don’t pay for transportation, nursing staff, or clinic overhead. You do pay for supplies (bags, catheters) and potentially a cycler machine. Many insurance plans cover these supplies at home. HD involves higher systemic costs due to labor and facility maintenance, though the patient rarely sees this directly unless they opt for home HD, which requires expensive water purification systems and space in your house.
Centers for Medicare & Medicaid Services (CMS) actively incentivize home dialysis. Their ESRD Treatment Choices Model aims to shift more patients toward home therapies because studies show better quality of life and lower hospitalization rates for stable patients.

Who Should Choose Which?
Let’s simplify the decision matrix based on patient profiles.
Choose Peritoneal Dialysis if:
- You want to avoid frequent travel to a clinic.
- You have a supportive partner or live alone but are self-motivated.
- You have unstable blood pressure or heart disease that doesn’t tolerate rapid fluid shifts.
- You want to preserve residual kidney function.
- You have a clean, dry space at home for supplies.
Choose Hemodialysis if:
- You prefer having professionals manage your treatment.
- You have limited abdominal space or history of abdominal surgeries.
- You lack the physical ability to perform sterile connections (poor vision/dexterity).
- You have strong social support for transport to the clinic.
- You prefer having two full days off per week.
Next Steps: Preparing for the Conversation
Don’t decide today. Take notes. Ask your nephrologist these specific questions:
- "Is my peritoneal membrane healthy enough for PD?" (They can test this.)
- "Do I have a suitable vein for an AV fistula?" (Ultrasound can check this.)
- "What is the local training program like for PD?" (Training takes 10-14 days.)
- "Are there home HD options available locally?" (This is a third option combining home convenience with HD clearance.)
Remember, you can switch modalities later. Many patients start with one and move to the other as their health or life circumstances change. The goal is to find the therapy that lets you live the best life possible while keeping you safe.
Can I switch from hemodialysis to peritoneal dialysis?
Yes, switching is possible. If you are currently on hemodialysis, you would need surgery to place a Tenckhoff catheter in your abdomen. You must wait 2-4 weeks for the incision to heal before starting PD. During this transition period, you continue hemodialysis. Discuss this with your care team well in advance to plan the surgical timing.
Which dialysis is less painful?
Peritoneal dialysis is generally considered less painful because it does not involve needles. Hemodialysis requires needle sticks into your fistula or graft twice per session, which can be uncomfortable. However, PD can cause abdominal discomfort or bloating due to the fluid volume, and peritonitis (if it occurs) is very painful. Most patients report PD as physically less invasive day-to-day.
Does peritoneal dialysis allow me to work?
Many PD patients return to work. Because treatments happen at home, often overnight with a cycler, you can maintain a standard 9-to-5 job. You may need flexible hours for occasional supply deliveries or clinic visits. Hemodialysis patients working in-center jobs often struggle with the 12-15 hours per week spent traveling and sitting in the clinic, plus recovery time.
How long can I stay on peritoneal dialysis?
There is no set limit. Some patients stay on PD for 10 years or more. Over time, the peritoneal membrane may become less efficient (fibrosis) or prone to infections. If your clearance rates drop or you experience recurrent peritonitis, your doctor may recommend switching to hemodialysis. Regular monitoring ensures you stay on PD as long as it remains effective.
Is home hemodialysis better than peritoneal dialysis?
Home hemodialysis offers high clearance similar to in-center HD but with more frequency (often 4-6 times a week). It provides excellent toxin removal and flexibility. However, it requires significant space for equipment, complex water treatment, and technical troubleshooting skills. PD is simpler logistically but offers slower, continuous filtration. The "better" option depends on whether you prioritize high-intensity cleaning (Home HD) or simplicity and continuity (PD).