
Most people think carpal tunnel syndrome is just a bad wrist ache that goes away with rest. But for millions, it’s a slow, creeping problem that starts with numb fingers at night and ends with dropped keys, weak grips, and trouble buttoning shirts. It’s not just discomfort - it’s nerve damage in motion. Carpal tunnel syndrome (CTS) is the most common nerve compression disorder in the upper body, affecting about 10% of the U.S. population. Women are three times more likely to get it than men, and the peak age is between 45 and 60. If you’ve ever woken up shaking your hand because your thumb and fingers felt like they were asleep, you’re not alone.
What Exactly Is Happening in Your Wrist?
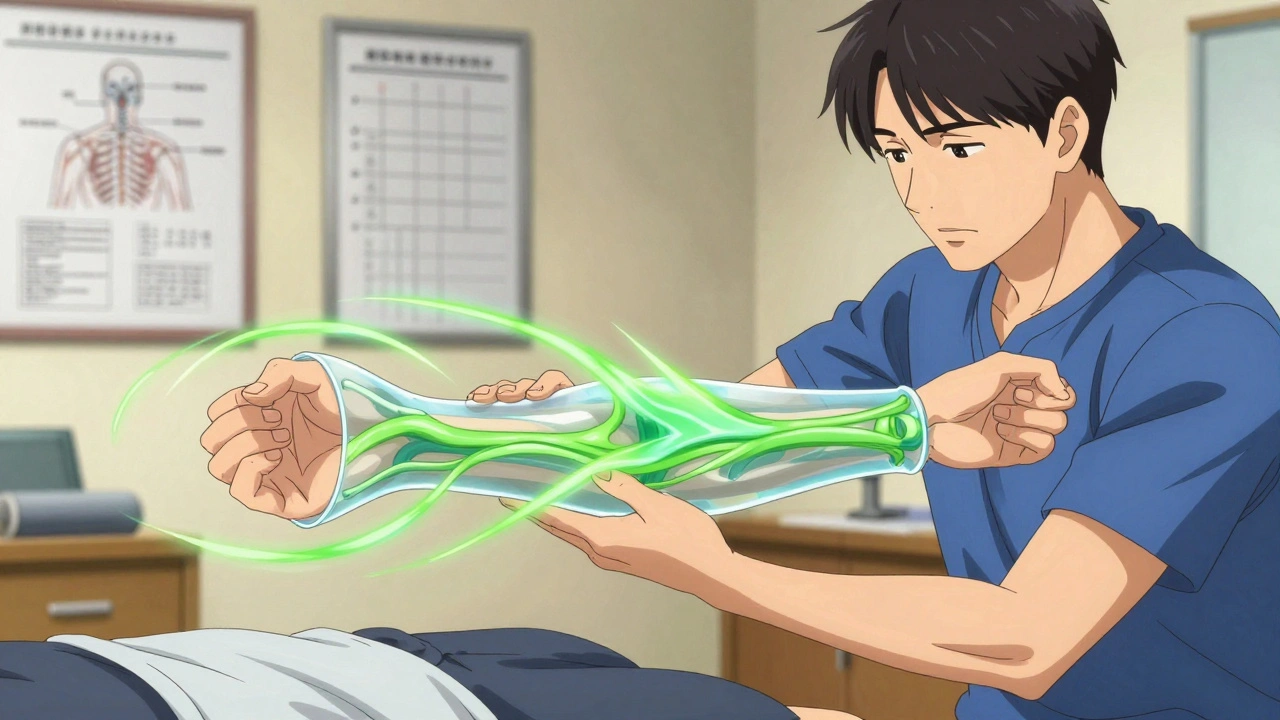
Your wrist isn’t just bone and skin. Inside it lies a tight tunnel made of bones on the bottom and a tough ligament on top. Nine tendons that bend your fingers and thumb squeeze through it, along with one critical nerve: the median nerve. This nerve controls sensation in your thumb, index, middle, and half of your ring finger. When that tunnel gets too crowded - from swelling, repetitive motion, or even just genetics - the median nerve gets squished.The pressure doesn’t just pinch the nerve. It cuts off its blood supply. Without proper circulation, the nerve starts to break down. First, it loses its ability to send clear signals - that’s the tingling and numbness. Then, over time, the nerve fibers themselves get damaged. If left untreated, this can lead to permanent muscle wasting in the thumb, known as thenar atrophy. That’s not something you can fix with a few days off work.
How Do You Know It’s Carpal Tunnel - Not Just a Bad Night’s Sleep?
Symptoms don’t come out of nowhere. They follow a pattern. In the early stage, you might only feel it at night. You wake up with your hand asleep, and shaking it helps. That’s classic. You might also feel it while driving, holding a phone, or reading a book. These are all positions where your wrist bends slightly, squeezing the tunnel even more.As it gets worse, the numbness and burning spread into the day. You start dropping things. Buttoning a shirt feels like a puzzle. You can’t feel the difference between a coin and a key in your pocket. By the time you’re struggling with doorknobs or opening jars, you’re in the severe stage. At this point, nerves are already damaged. Muscle strength is fading. Waiting longer makes recovery harder.
Doctors don’t just guess. They use specific tests. The Phalen test - holding your wrists bent for a minute - can trigger tingling if CTS is present. The Tinel sign - tapping over the nerve - causes an electric shock feeling down the fingers. The carpal compression test, where pressure is applied directly over the tunnel, also reproduces symptoms. For confirmation, nerve conduction studies measure how fast signals travel through the median nerve. If the signal slows down past 3.7 milliseconds, it’s a clear sign of compression.
Conservative Treatments: The First Line of Defense
If you’re in the early or moderate stage, surgery is not your first step. In fact, most people get better without it. The most effective non-surgical treatment? A wrist splint worn at night.Wearing a splint keeps your wrist straight while you sleep - no bending, no squeezing. Studies show 60-70% of people with mild to moderate CTS see major improvement after just 4-6 weeks of consistent use. It’s simple, cheap, and safe. But it only works if you wear it every night. Skipping nights? You’re not helping.
Another proven method is nerve gliding exercises. These aren’t stretches for your muscles - they’re gentle movements designed to help the median nerve slide freely through the tunnel. Doing them daily for 6-8 weeks can reduce pressure and improve symptoms. Physical therapists often teach these in 2-4 sessions.
Corticosteroid injections are another option. A shot of anti-inflammatory medicine into the carpal tunnel can reduce swelling and give relief for 3-6 months. About 70% of patients benefit. But it’s not a cure. It’s a pause button. If symptoms return after the injection wears off, you’re back to square one - unless you change what’s causing the problem.
Activity changes matter too. Avoid bending your wrist more than 30 degrees. If you type all day, raise your keyboard so your wrists stay neutral. Use voice-to-text. Switch hands when possible. If you work in manufacturing, healthcare, or food service - the top three industries for CTS - your job is likely part of the problem. Ergonomic adjustments aren’t optional; they’re necessary.
When Surgery Becomes Necessary
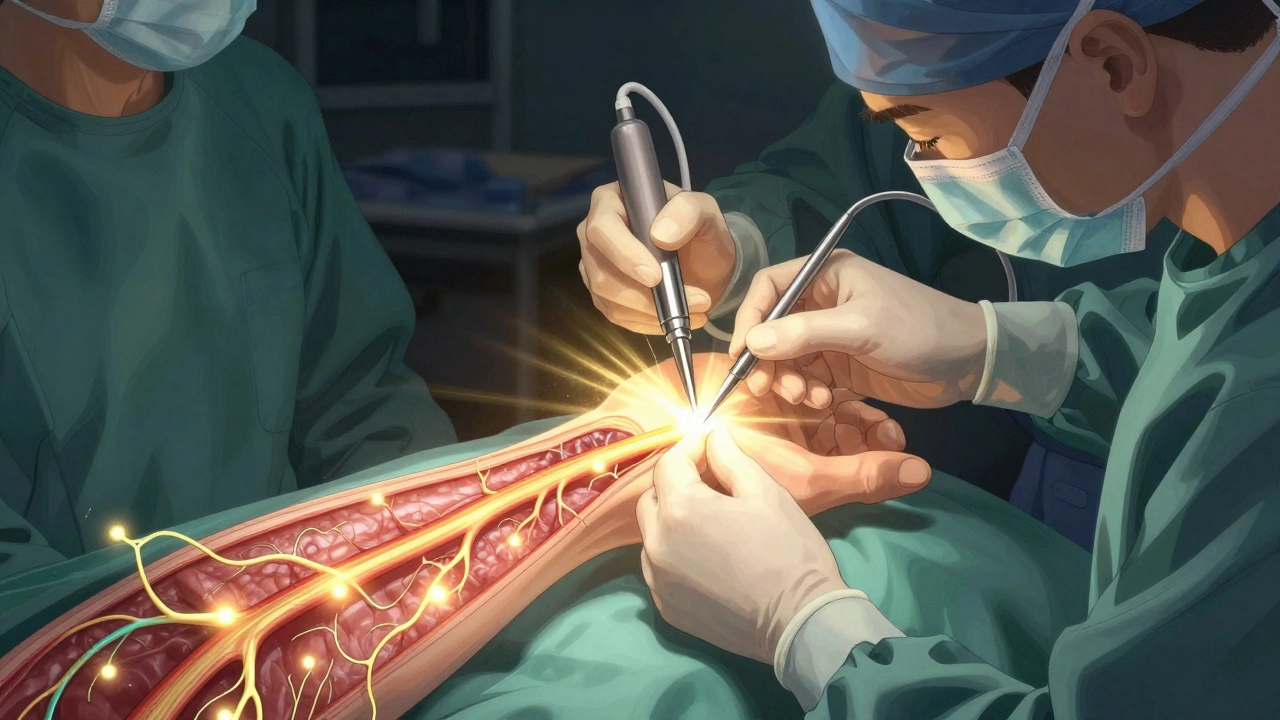
If you’ve tried splinting, exercises, and injections for 6-8 weeks with no improvement - or if you’ve lost muscle strength in your thumb - it’s time to consider surgery. The goal? Cut the ligament pressing on the nerve. That opens up the tunnel and gives the nerve room to heal.There are two main types: open release and endoscopic release. Open release involves a 2-inch incision on the palm. Endoscopic uses one or two tiny cuts and a camera to guide the cut. Both are highly effective, with success rates of 90-95%. The American Society for Surgery of the Hand reports most patients regain full function.
But surgery isn’t risk-free. About 15-30% of people get pillar pain - tenderness on the sides of the palm near the incision. Scar tenderness happens in 5-10%. Nerve injury is rare - less than 1% - but it can happen. Recovery takes time. Most people return to light work in 2-3 weeks. For heavy lifting or manual labor, you’ll need 6-12 weeks.
There’s a new option: ultrasound-guided percutaneous release. Approved by the FDA in 2021, this minimally invasive technique uses a tiny knife guided by real-time ultrasound. It’s less painful, and patients return to work 50% faster than with traditional surgery. It’s not available everywhere yet, but it’s growing fast.
Cost, Recovery, and What Insurance Covers
Conservative care - splint, therapy, injection - typically costs between $450 and $750 out of pocket. A custom splint runs $150-$250. Physical therapy sessions are $100-$200 each. A steroid injection is $300-$500. Most insurance covers these.Surgery is more expensive. With private insurance, you’ll pay $1,200-$2,500 out of pocket. Endoscopic surgery costs 15-20% more than open release, but recovery is faster. Without insurance, surgery can hit $8,000-$12,000. Post-op rehab usually includes 6-8 physical therapy sessions over 4-6 weeks.
Time off work depends on your job. Office workers often return in 2-3 weeks. Factory workers or those using power tools need 10-12 weeks. The key? Don’t rush. Returning too early can delay healing or cause re-injury.
Why Early Action Makes All the Difference
Here’s the hard truth: CTS gets worse the longer you wait. Patients with symptoms under 10 months have a 75% chance of improvement with conservative care. Those with symptoms over 12 months? Only 35%. Once the nerve is permanently damaged, no splint, no injection, no surgery can fully restore it.Studies show that early intervention - splinting, activity changes, and nerve gliding - cuts the risk of needing surgery by 45% within two years. That’s huge. It’s not just about avoiding pain. It’s about keeping your hands functional for life.
And here’s something surprising: up to 20% of people over 60 show abnormal nerve test results even when they have no symptoms. That means a test alone doesn’t diagnose CTS. Your symptoms, your daily life, your physical exam - those matter more than any machine reading.
What to Do Right Now
If you’re experiencing nighttime numbness or tingling in your thumb, index, or middle finger:- Buy a wrist splint (available at pharmacies or online) and wear it every night.
- Start doing nerve gliding exercises - search for "CTS nerve glides" and follow a video guide.
- Adjust your workstation: keep your wrists straight while typing, use an ergonomic keyboard, take breaks every 30 minutes.
- See a doctor if symptoms last more than 2 weeks or if you start dropping things.
- Don’t wait for pain to get worse. Nerve damage is silent until it’s too late.
CTS isn’t a fluke. It’s a warning. Your body is telling you something’s wrong. Listen early. Act fast. Your hands will thank you.
Suzanne Johnston
December 9, 2025 AT 00:01It’s wild how we’ve normalized suffering until it’s too late. Carpal tunnel isn’t just a wrist issue-it’s a symptom of a culture that treats bodies like disposable machines. We’re told to push through pain, to ‘just adapt,’ but nerves don’t adapt. They break. And then we wonder why we can’t hold a coffee cup anymore. This post is a quiet rebellion against that mindset.
George Taylor
December 10, 2025 AT 07:02Wow. So much text. Where’s the TL;DR? Also, who says ‘thenar atrophy’ like it’s a cool word to drop? I just want to know if I need to quit my job or not.
Elliot Barrett
December 11, 2025 AT 18:50Typical medical article. Ignore the 10% stat-most of those people are just lazy and type too much on their phones. If you’re not a factory worker, you’re probably imagining this.
Maria Elisha
December 12, 2025 AT 19:29Same. Woke up with numb fingers yesterday. Bought a splint on Amazon. 10 bucks. Wearing it tonight. Fingers still kinda tingly but whatever.
Andrea Petrov
December 13, 2025 AT 08:34Did you know the FDA approved this ‘ultrasound-guided release’ because Big Pharma wanted to replace corticosteroids? They’re pushing minimally invasive stuff because injections don’t have enough profit margin. Also, ergonomics? Please. Your ‘neutral wrist’ is just corporate propaganda to avoid paying for better chairs. They don’t care if you lose function-they care about your productivity metrics.
And don’t get me started on nerve gliding exercises. Those are just placebo stretches designed to make you feel like you’re doing something while the real solution-removing your wrist from repetitive motion-isn’t even on the table.
They’ll tell you surgery is 95% effective. But what they don’t say is 30% of people get chronic pain afterward. And who pays for that? You. Your insurance won’t cover therapy for phantom pain from a ‘successful’ surgery. It’s all a loop.
And why do they say women are 3x more likely? Because they’re more likely to report symptoms. Men just keep typing until their hands give out. Then they blame it on ‘aging.’
I’ve seen this pattern. Every time a new ‘miracle cure’ comes out, it’s just a repackaged version of the same thing. Splints? Been around since the 80s. Steroids? 70s. Surgery? 50s. They just change the name and the price tag.
And don’t tell me to ‘listen to my body.’ My body’s been screaming since 2018. Nobody listens until you can’t grip your own child’s hand.
Graham Abbas
December 15, 2025 AT 03:47Andrea, you’re not wrong-but you’re also not helping. There’s truth in the system’s exploitation, yes. But dismissing every intervention because of corporate motives is like refusing to take aspirin because Big Pharma invented it. We’re not arguing about capitalism here-we’re talking about a nerve that’s being crushed in real time.
Maybe the splint isn’t a cure. Maybe the surgery isn’t perfect. But if I can hold my daughter’s hand again without pain? I’ll wear the splint. I’ll do the exercises. I’ll take the shot. I’ll even get the ultrasound-guided cut if it means I don’t become a ghost of my own hands.
It’s not about trusting the system. It’s about surviving it.
William Umstattd
December 16, 2025 AT 03:03You’re both wrong. And I’m not being petty-I’m being precise. The term is ‘thenar eminence atrophy,’ not ‘thenar atrophy.’ The thenar is a group of muscles; the eminence is the mound they form. You’re not a neurologist if you can’t get the anatomy right.
Also, ‘carpal compression test’ isn’t a standardized term-it’s ‘Phalen’s and Tinel’s’ are the accepted clinical signs. The ‘carpal compression test’ is colloquial. And the 3.7 millisecond threshold? That’s for motor latency, not sensory. You’re conflating two different metrics.
This article reads like a marketing brochure for a physical therapy clinic. Half the claims are oversimplified. The rest are dangerously misleading. I’ve reviewed 37 CTS studies this year. None of them support the ‘75% improvement under 10 months’ stat without controlling for age, BMI, and comorbidities.
And don’t get me started on ‘nerve gliding exercises.’ The evidence is weak. A 2021 Cochrane review found no clinically significant benefit over placebo. But you’ll see it everywhere because PTs need to justify their sessions.
Yes, splints work. Yes, steroids help. But if you’re going to write a 2,000-word piece, at least get the science right. Otherwise, you’re just feeding misinformation under the guise of ‘awareness.’
Chris Marel
December 17, 2025 AT 08:09Thank you for writing this. I’m from Nigeria, and here, people think hand pain is just ‘bad luck’ or ‘spiritual.’ No one talks about nerves or tendons. I showed this to my cousin who works in a textile factory-she’s been ignoring her numb fingers for two years. She’s going to the clinic tomorrow. I don’t know if this will fix her, but at least now she knows it’s not ‘normal.’ That’s worth something.